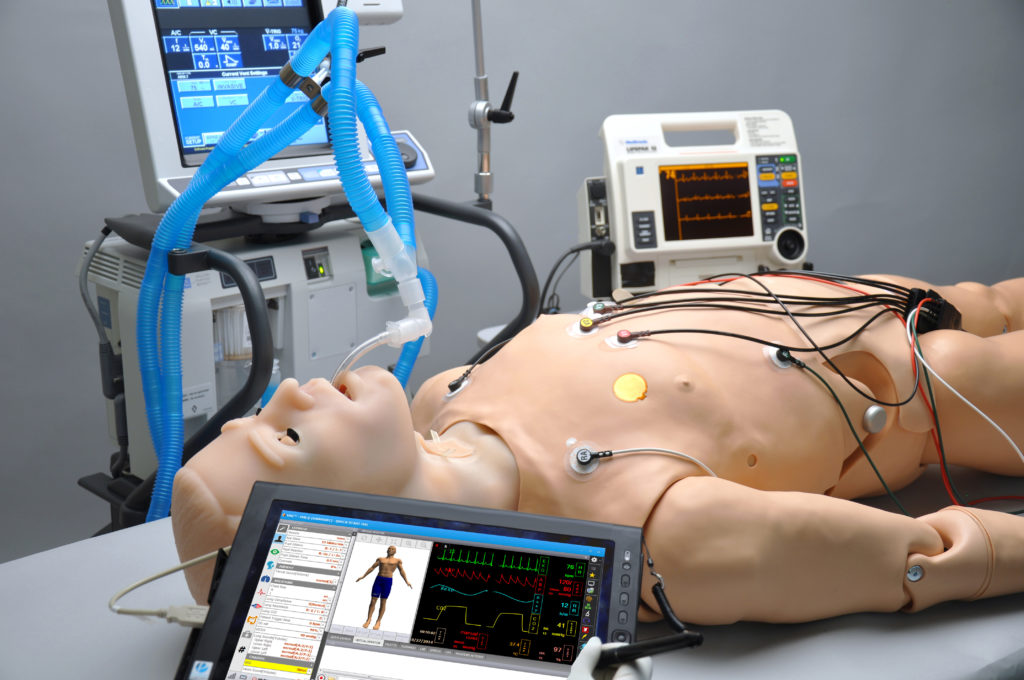
Among the uses for robotics in healthcare is in safely training medical personnel. This is especially important with ventilator shortages during the COVID-19 pandemic. Gaumard Scientific has created HAL, a robotic patient simulator that can be intubated and attached to an actual ventilator.
The Miami-based company has spent years improving its simulator mannequins and is working to meet increased demand during the novel coronavirus crisis, said Jim Archetto, vice president of corporate planning at Gaumard.
“It’s similar to a flight simulator,” he told The Robot Report. “These systems are designed to allow physicians and first responders to practice and prepare before getting into live situations. It’s best to practice for high-risk, low-frequency problems that they may not see in training.”
Realistic robotic response
“Residents don’t get the clinical time they used to, and with COVID-19, rapid training is essential, with general practitioners moving into critical care and nurses moving into intensive care,” Archetto said. “They all need to be prepared.”
Gaumard makes several realistic humanoid robots that are capable of producing vital signs that standard monitors can read.
“These basic trainers have arms with synthetic veins,” said Archetto. “First responders must determine anaphylaxis from a seizure, a bee sting, or epilepsy. When a patient comes into an emergency room, certain assessments need to take place — blood pressure, breathing, pupil dilation. The simulator’s chest can rise and fall, and its pupils dilate.”
“Our simulators can be intubated and respond on a ventilator as a human would,” he added. “They can mimic complications, with increased resistance. We can also duplicate COVID-19 symptoms.”
Design avoids distraction
Gaumard’s simulators are designed to be realistic in their physical responses, if not as much in facial appearance and variety, Archetto acknowledged. “We discussed it quite a bit,” he said. “They have to be realistic, but we really want the best teaching tool to ensure competency in respiratory care.”

A pediatric HAL S2225 on mechanical ventilation. Source: Gaumard
“When a healthcare worker gets into complex scenarios, they’re focused on the robot as a patient, and an instructor can remotely talk for them via a headset,” Archetto explained. “The learner is engaged and focused on the clinical aspects rather than the ‘uncanny valley.'”
“In design meetings, we decided on three skin tones,” he said. “There are good clinical reasons to have different skin tones. It can be hard to see jaundice or cyanosis with darker skin tones. We wanted to reflect different ethnicities without offending, alienating, or distracting customers and learners.”
Gaumard provides simulator options
There are several models of HAL, including pregnant women, trauma patients, and children.
“Body mass varies, and there are very specific treatments that go with weight,” Archetto said. “Workers need to know how to move a 150-lb. pregnant female. Our 5-year-old is in the 50th percentile, and the newborn is 8.5 lb. Adult males are a bit lighter than reality, and we offer just torsos for critical care simulation. The military wants heavier bodies, so we add weighted vests.”
“HAL for trauma comes with full limbs, as well as amputated limbs for military training,” Archetto said. “Medics can learn how to treat someone with aortic bleeding from an IED [improvised explosive device]. There is a module with a reservoir of artificial blood, and the system responds to tourniquet pressure, and the blood pressure changes.”
“For birthing simulation, Victoria can train on performing a C-section,” he said. “Gaumard recently introduced a mixed-reality concept for shoulder dystocia, when a baby gets stuck behind the pubic bone. With a Microsoft HoloLens 2, students can learn how to recognize it and successfully deliver the baby. Many young people are avid gamers and are comfortable in augmented and virtual reality. In our training, there’s also the tactile element.”

The Victoria simulator can train for complications in childbirth. Source: Gaumard
Training robots need to be rugged
Not only must the simulators accurately replicate symptoms, but they also have to be rugged for multiple trainees.
“These simulators have to be reliable and work day after day. Our operators are not engineers like those at Hanson Robotics supporting Sophia,” Archetto noted, referring to the celebrity humanoid robots. “For example, at professional societies such as the American College of Emergency Physicians, which has two Victorias, each one will deliver 60 times a day.”
“Trauma HAL gets dragged through the mud and dirt, and it can be hosed down,” he said. “The point is that learners have to be able to make mistakes on these robots so they don’t in real life.”
HAL has a modular design and realistic responses. Source: Gaumard
Cameras, tablets assist in training
As with industrial workcells and other forms of automation, Gaumard’s Care in Motion offering uses cameras to monitor and record all aspects of medical response, including human performance and workflows.
“They’ll learn through the process, but after a scenario, educators will debrief them based on what went well or didn’t go well in the simulation,” Archetto said. “It runs on a Microsoft Surface Pro, which is wireless. Emergencies don’t always take place in hospitals, so you can mount the camera in the back of an ambulance, on an IV pole on a stretcher, or carry it around.”
“The Omni 2 is a more basic tablet for controls for Code Blue, maybe in a firehouse rather than a hospital,” he said. “All the simulators are controlled with tablets or Surfaces, from the adult and pediatric HAL to Victoria. They can run pre-programmed scenarios, such as a dislocated shoulder or a baby stuck in delivery. They will run automatically, or the instructor can change things on the fly, such as cause a drop in blood pressure.”
Vertical integration helps Gaumard guarantee ROI
While various institutions will measure their return on investment (ROI) differently, Archetto said Gaumard’s simulators quickly justify themselves.
“We do some risk management. As with flight simulators, institutions invest in these trainers to give muscle memory on real equipment,” he said. “A 12-lead EKG [electrocardiogram] will work with our simulator. The benefit is that when a real patient comes in, the person knows what to do. It can be measured in time to result — with an EKG, it’s a number of minutes.”
“Vertical integration keeps costs low. We have vertically integrated design, development, and manufacturing at our headquarters in Miami,” said Archetto. “We have a sculptor who creates faces and molds with the electromechanical elements inside.”

Instructors can monitor procedures such as stabilization. Source: Gaumard
“Gaumard also has different models for different centers’ training objectives,” he said. “Noelle 550 is a basic model that is less realistic than Victoria. It ranges from $15,000 to $65,000. At the same time, we have a birthing model that is just the torso for $3,000.”
“Our price point has the lowest capital investment and operating cost over a five-year period compared with that of competitors,” claimed Archetto. “HAL with Serial No. 08 has been operating for 12 years.”
Gaumard also offers a variety of service plans, from “Bronze” to “Platinum Plus.” “Every medical school, hospital, or firehouse has a different training program,” Archetto said. “We don’t offer closed-end leases or trade-in programs, but we do have financing, and we can provide loaners so there are no gaps in training.”
Gaumard keeps up with changes
“COVID-19 has changed medical education quite a bit,” Archetto said. “We are constantly assessing how educators train and students learn. A lot had already changed in the past 10 years, and students are extremely comfortable with tablets and mixed reality, which is a change.”
“Tetherless realism is very important, because emergencies can happen anywhere,” he said. “Gaumard’s simulators work with real pulse oximeters, ventilators, fetal heart monitors, and contraction monitors and provide real results. Otherwise, with low-frequency, high-risk scenarios, trainees may see a rare complication only once in a three-month rotation.”




Tell Us What You Think!